
Achilles Tendon Disorders
Achilles Tendinitis/Tenosynovitis
NON-SURGICAL MANAGEMENT
Achilles tendon injuries are a common foot problem. It usually causes pain, stiffness and swelling near where the tendon inserts into the heel. It can start slowly, and develop over a period of time.
There can be a few reasons why people may develop this problem:
Overuse - such as runners
Training or exercising with inappropriate shoes
Poor running technique or changing your running program
Biomechanics of the lower-lib and foot
Genetics
The condition is also noted more commonly in patients who have high blood pressure, high cholesterol and/or diabetes. Very rarely the condition can be brought on taking antibiotics called ciprofloxacin and ofloxacin.
The condition occurs in about 6 in 100 inactive people in their lifetime but is more common in athletes.
There are four common causes for pain in region near the back part of the heel:
Paratenosynovitis: - Inflammation of the sheath surrounding the Achilles tendon, rather than of the tendon itself.
Non-insertional Achilles tendonitis: - In this, type the pathology is typically located 2-6cm above the insertion of the Achilles tendon to the heel bone.
Insertional Achilles tendonitis: - In this type, the pathology is located at the insertion of the Achilles tendon to the heel bone. Sometimes it is caused by inflammation of a bursa at the back of the heel.
Achilles tendon rupture: - Rupture of the Achilles tendon, usually 2-6cm from the insertion to the heel bone, may not be clinically obvious and may be confused with tendonitis
Achilles tendonitis is often associated with an increase in activity level such as starting a new training regimen or attempting to resume a normal activity level. Irritation to the synovial sheath that encloses the Achilles tendon is thought to be caused either by direct pressure from shoe wear or from an irregularity in the Achilles tendon. The Achilles tendon is believed to suffer microtearing when it is overloaded, and the body’s healing response to this microtearing may also contribute to symptoms. Despite the pain originating from the Achilles tendon, the tendon itself is usually intact, and the presence of Achilles tendonitis is not believed to increase the risk of an Achilles Tendon rupture.
Basic treatment includes rest, ice, topical anti-inflammatories, stretching, orthotics, physiotherapy, Extracorporeal shock wave, PRP injections and surgery. There is some thought that modifying factors such as high cholesterol, hypertension and weight loss might also facilitate recovery.
Most patients with Achilles tendonitis can be treated effectively with non-operative treatment. This usually involves a period to let the symptoms settle, followed by a gradual return to normal activities. The elements of non-operative treatment may include:
Activity Modification
In the short term, it may be necessary to stop any precipitating activities. Precipitating activities include high impact exercises that cause weight to be placed on the front part of the foot. This includes running, jumping, walking up hills and repetitive stair climbing. New training programs should be reviewed and stopped, at least until the symptoms resolve.
Shoe Wear Modification
It is important to avoid shoes that precipitate or aggravate symptoms. In general, using well fitted "comfort" shoes will be beneficial. Some shoe modifications may also be helpful. Some patients will feel more comfortable in shoes with a slight heel, or with the addition of a heel lift inside the shoe. An increased heel height will tend to take some of the load off of the Achilles tendon. Patients should avoid shoes with a "Negative Heel" (i.e. the heel height is lower than the forefoot height) as this has been shown to increase the force through the Achilles, often leading to the development of Achilles tendonitis. Aggravating shoes should be modified or discarded so that they do not cause an increase or recurrence of symptoms.
Medications
Anti-inflammatory medications taken 1-3 times per day can help to settle symptoms in the short term, and break the cycle of pain and discomfort. However, for successful long-term management, NSAIDs usually need to be combined with other non-operative treatment strategies
Calf and Achilles Stretching
A tight calf muscle will increase the force going through the Achilles tendon and predispose the tendon to micro-tearing. A consistent calf stretching program is an important part of treatment. (Figure 3)
Double leg heel rises
A high repetition, low resistance calf strengthening program can be very helpful in stretching and strengthening the Achilles tendon and calf muscle. Double leg heel rises, done in a controlled manner and performed while standing on the edge of stairs, (to allow for more movement through the ankle) can be very helpful. Consider starting with 5 sets of 5 repetitions and slowly over a period of weeks advance to 10-15 sets of 15 repetitions.
Eccentric Achilles Tendon Exercises (ex. Heel Drops)
Controlled exercises where the Achilles tendon is being lengthened while the calf muscle contracts have been shown to be very helpful in improving the symptoms associated with Achilles tendonitis. An example of this type of exercise is a "Heel drop", where the patient stands on their toes while positioned on the edge of a ledge, such as a stair. They then slowly lower their heels down below the ledge, simultaneously stretching and strengthening the Achilles tendon. This can be done with both legs at the same time (bilaterally) or for a more concentrated effort, one leg at a time. It can also be done with the knees straight (putting force on the gastrocnemius) or with the knees bent (putting force on the soles). Patients should gradually work up to performing 5 sets of 10 repetitions. These exercises should be performed 5-6 days per week during the active treatment phase, and then 3 times per week to minimise the chance of developing recurrent symptoms. It is critical that this exercise be approached cautiously, as it has the potential to put excessive pressure on the Achilles. Patients should always warm up first (ex. get their blood flowing on an exercise bike for 5-10 minutes) before performing these exercises.
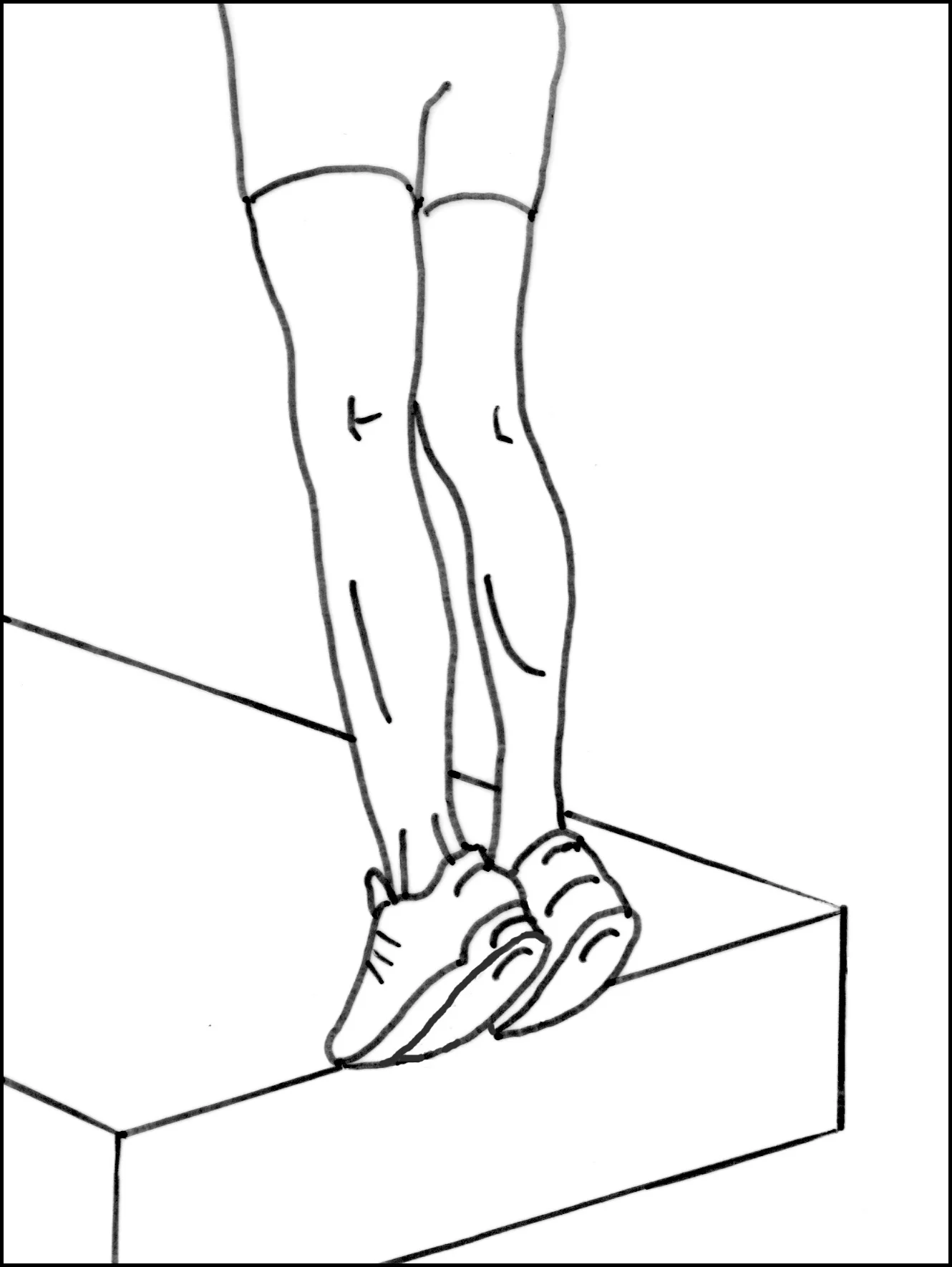
Fig 1.

Fig 2.

Fig 3.
PRP injections
It has been proposed that injecting plasma-rich protein (PRP), taken from the patients’ own blood, may stimulate healing. However, there is a lack of evidence supporting that notion that PRP injections are more effective than traditional treatment options --or even when compared to placebo treatments and this can be discussed with you during your consultation.
Extracorporeal Shock Wave Lithotripsy (ESWL) is another treatment modality to help this problem. It is a non-invasive treatment in which a device is used to pass acoustic shockwaves through the skin to the affected area.